@juk , look.
I'll be the first to say that vaccinating with single target spike protein vaccines for mRNA viruses which are constantly mutating may not be the best long-term solution to the situation, because you can never keep up with the mutations.
When I see those graphs from the non-peer reviewed preprint article (you might link those for us when you quote them) you posted,
Background The purpose of this study was to evaluate whether a bivalent COVID-19 vaccine protects against COVID-19. Methods Employees of Cleveland Clinic in employment on the day the bivalent COVID-19 vaccine first became available to employees, were included. The cumulative incidence of...

www.medrxiv.org
[It is a Cleveland Clinic study of generally healthy individuals who were employees, some of whom were working in high-risk environments, average age of 42. It is not a study of the general population and excludes many of the highest risk groups.]
Here is what the authors conclude, despite the confounding findings in the graph you posted:
Here is what I think: the people who are most likely to vaccinate are those who are or who perceive themselves to be at higher risk. This is not only underlying conditions but also higher risk environments. Not all, but many. Therefore, there is a self-selection process going on that may skew the data to what you are seeing.
This same self-selection could be affecting the hospitalization data you brought us above with your incredibly high relative risk numbers.
In addition, it is important to remember that at this time, we are counting the people hospitalized
with covid the same as people hospitalized
for covid. That number is not insignificant.
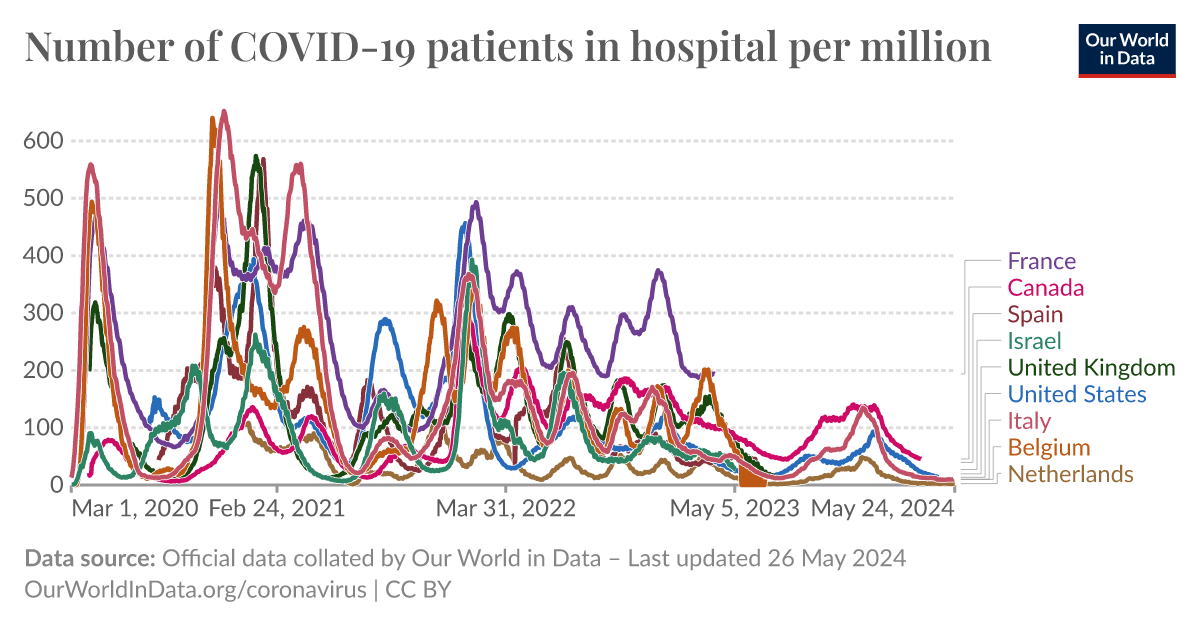
Furthermore, hospitalizations for Covid are RARE. Here is a comparative graph for hospitalizations per million showing the variations. With the exception of France, it is in the range of 100 per million during peaks, and much lower much of the rest of the time.
An interactive visualization from Our World in Data.

ourworldindata.org
View attachment 887485
Given the low numbers, possibly cut in half by coincident infection, it is hard to draw conclusions about causation from vaccination. People who are at higher risk for covid are also at higher risk for other conditions that might hospitalize them (older, diabetic, obese, arthritic, etc).
I want to see a prospective paper that studies matched patients who are of comparable risk in terms of underlying conditions and age, and that excludes prior infection (which is a confounding variable and may be hard to determine) then compares vaccinated to nonvaccinated for subsequent covid infection and hospitalization due to Covid. Then I might entertain your idea that vaccination causes disease. Not saying it couldn't be a thing, but your examples don't show that. There are other explanations.