The US is 16% of those deaths, wildly overrepresented. Why would anyone listen to the US official line?Although it is a different virus and a different time, I think it is interesting to compare the 1918 flu epidemic to the current Covid pandemic.
The flu pandemic is estimated to have killed 1% of the world population in 3 years. So far 0.08% of the world population have lost their lives due to Covid. Best estimates I can find.
Some people have said here that we are doing worse with Covid than that flu pandemic at this point. I am not sure how they get there, unless flattening the curve (AKA keeping people alive longer) is a bad thing. In those people's minds.



Welcome to Tesla Motors Club
Discuss Tesla's Model S, Model 3, Model X, Model Y, Cybertruck, Roadster and More.
Register
Install the app
How to install the app on iOS
You can install our site as a web app on your iOS device by utilizing the Add to Home Screen feature in Safari. Please see this thread for more details on this.
Note: This feature may not be available in some browsers.
-
Want to remove ads? Register an account and login to see fewer ads, and become a Supporting Member to remove almost all ads.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Coronavirus
- Thread starter Wenche
- Start date

DanCar
Active Member
1918 flu pandemic - killed young and oldAlthough it is a different virus and a different time, I think it is interesting to compare the 1918 flu epidemic to the current Covid pandemic.
The flu pandemic is estimated to have killed 1% of the world population in 3 years. So far 0.08% of the world population have lost their lives due to Covid. Best estimates I can find.
Some people have said here that we are doing worse with Covid than that flu pandemic at this point. I am not sure how they get there, unless flattening the curve (AKA keeping people alive longer) is a bad thing. In those people's minds.
Covid - Mostly the elderly and those with comorbidities. The healthy got / get a bad cold. The young pass it onto others.
Very true, with some exceptions.1918 flu pandemic - killed young and old
Covid - Mostly the elderly and those with comorbidities. The healthy got / get a bad cold. The young pass it onto others.
Well, there's long covid, too. Gotta throw that in, and not just for grandma, who died and so didn't get it.
Older age above 30 years was associated with a higher risk of reporting long COVID symptoms in the univariate analysis; however, after adjusting for baseline covariates, older age was associated with a lower risk, with those aged 30–39 years having a 6% lower risk (0.94, 0.90–0.97) and those aged ≥70 years having a 25% lower risk (0.75, 0.70–0.81) compared to those aged 18–30 years.
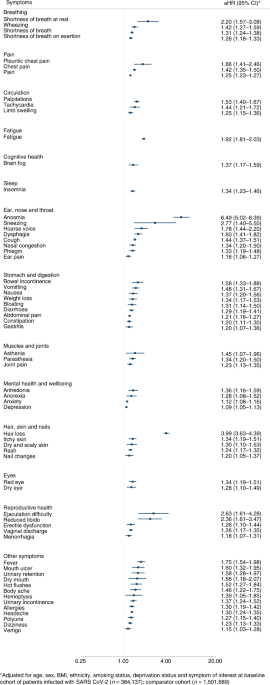
Symptoms and risk factors for long COVID in non-hospitalized adults - Nature Medicine
A retrospective analysis of primary care records in the United Kingdom reveals individual symptoms associated with SARS-CoV-2 infections, which persisted for 12 weeks or more after infection, as well as risk factors associated with developing long COVID.
 www.nature.com
www.nature.com
Of course, as with currently, if patients were treated they faired much better.Very true, with some exceptions.
Well, there's long covid, too. Gotta throw that in, and not just for grandma, who died and so didn't get it.
Symptoms and risk factors for long COVID in non-hospitalized adults - Nature Medicine
A retrospective analysis of primary care records in the United Kingdom reveals individual symptoms associated with SARS-CoV-2 infections, which persisted for 12 weeks or more after infection, as well as risk factors associated with developing long COVID.
But what did we do, we changed our practices to withhold treatment.

THE TREATMENT OF "SPANISH INFLUENZA"
To the Editor: —In a number of cases of influenza and influenzal pneumonia, seen both in my private practice and at the Alexian Brothers' Hospital, I have used a treatment from which my results have been most satisfactory.The clinical course of the condition may be divided for convenience...
 jamanetwork.com
jamanetwork.com
Last edited:
PACEMD
Active Member
Ehh.......ya kids today.......ya don no notin'........Well back then men were men and they didn't wear no stinking masks. They just sucked in the virus and they enjoyed it.
PACEMD
Active Member
Others might say you made that sh*t up. Just sayin'.......Without evidence that americans were more susceptible, some might say it's iatrogenic. In fact some are.
PACEMD
Active Member
Well, not entirely. With the first several seasons or three of covid, true enough it tended to mostly spare pediatric patients and was in fact statistically more likely to be severe in the elderly and/or those with other medical illnesses, but that was far from the whole story. During those rounds, for an individual presenting with covid pneumonia, meaning what killed during those rounds, other than statistics we had no way to predict who would progress to severe illness or death and who would slide on through. I had many young, healthy, 30-40+ year-olds, for example, who appeared not so bad initially but who did not survive and at the same time many elderly folks with extensive comorbidities who just marched on through.1918 flu pandemic - killed young and old
Covid - Mostly the elderly and those with comorbidities. The healthy got / get a bad cold. The young pass it onto others.
Early on, for example, a 75-year-old with an LVAD and a nasty-looking chest Xray, did fine and with little help, same with a bilateral lung transplant 40-year-old. We also had quite a few folks in their 30s-40s+, young and healthy otherwise, who either did not survive or if they did only after a protracted hospital course.
The truth is, other than statistics, which do not apply to the individual except in a doesn't really help best-guess manner, we had no way to predict morbidity/mortality in the individual. That means susceptibility is not yet understood. I would guess a genetic factor not yet identified and/or viral load/timing, or something else entirely. In general with such things, it's often a combination of factors. Truth is we still know very little about this disease. But that's not even close to surprising, it is in fact pretty much normal for the process. What is surprising is how quickly we have progressed in that understanding. That mostly as a side effect of the now many years of efforts invested in viral research for HIV and hepatitis C. This rapid progression always has advantages and disadvantages. The disadvantage manifests as much of the evident confusion and chaos kicked around.....
Yes. 40-year-old perfectly (as far as anyone can tell) woman, mother of 2 young kids, nonsmoker, dies of fulminant Covid cardiomyopathy. 61-year-old male smoker, spends 2 months in the hospital with Covid pneumonia, discharged in a wheelchair on max home oxygen because he cannot even walk across the room, he's so short of breath. 1 year later he's hiking into high mountain lakes. Still a great mystery who survives and who doesn't.Well, not entirely. With the first several seasons or three of covid, true enough it tended to mostly spare pediatric patients and was in fact statistically more likely to be severe in the elderly and/or those with other medical illnesses, but that was far from the whole story. During those rounds, for an individual presenting with covid pneumonia, meaning what killed during those rounds, other than statistics we had no way to predict who would progress to severe illness or death and who would slide on through. I had many young, healthy, 30-40+ year-olds, for example, who appeared not so bad initially but who did not survive and at the same time many elderly folks with extensive comorbidities who just marched on through.
Early on, for example, a 75-year-old with an LVAD and a nasty-looking chest Xray, did fine and with little help, same with a bilateral lung transplant 40-year-old. We also had quite a few folks in their 30s-40s+, young and healthy otherwise, who either did not survive or if they did only after a protracted hospital course.
The truth is, other than statistics, which do not apply to the individual except in a doesn't really help best-guess manner, we had no way to predict morbidity/mortality in the individual. That means susceptibility is not yet understood. I would guess a genetic factor not yet identified and/or viral load/timing, or something else entirely. In general with such things, it's often a combination of factors. Truth is we still know very little about this disease. But that's not even close to surprising, it is in fact pretty much normal for the process. What is surprising is how quickly we have progressed in that understanding. That mostly as a side effect of the now many years of efforts invested in viral research for HIV and hepatitis C. This rapid progression always has advantages and disadvantages. The disadvantage manifests as much of the evident confusion and chaos kicked around.....
Slipstream
Member
Educational Messaging Increases COVID-19 Vaccine Acceptance and Uptake
The results of the study found that delivery of COVID-19 vaccine messaging platforms resulted in appreciably higher vaccine acceptance among intervention group participants compared with the control group (25.8% vs 12.0%) as well as uptake within 30 days (20% vs 8.7%). The impact of the intervention was greater in Latinx persons and participants without primary care physicians.
“Results of this cluster randomized clinical trial showed that with low NNT (number needed to treat), implementation of COVID-19 vaccine messaging platforms in EDs leads to greater vaccine acceptance and uptake in unvaccinated ED patients,” the researchers concluded. They added that broad implementation (of messaging) in EDs “could lead to greater COVID-19 vaccine delivery to underserved populations whose primary health care access occurs in EDs.”
AlanSubie4Life
Efficiency Obsessed Member
Of course, as with currently, if patients were treated they faired much better.
But what did we do, we changed our practices to withhold treatment.
View attachment 889850THE TREATMENT OF "SPANISH INFLUENZA"
To the Editor: —In a number of cases of influenza and influenzal pneumonia, seen both in my private practice and at the Alexian Brothers' Hospital, I have used a treatment from which my results have been most satisfactory.The clinical course of the condition may be divided for convenience...
Yep, definitely good to keep those bowels clear. Nothing like a brisk flushing to keep the temperature down. Do a colonoscopy while you’re at it, 2 for 1.
Only very slight mortality in the dying group! Excellent result.
You're confusing education with propaganda. If education had the effect you're claiming then more and more doctors would not be coming out calling to stop the shots.Educational Messaging Increases COVID-19 Vaccine Acceptance and Uptake
The results of the study found that delivery of COVID-19 vaccine messaging platforms resulted in appreciably higher vaccine acceptance among intervention group participants compared with the control group (25.8% vs 12.0%) as well as uptake within 30 days (20% vs 8.7%). The impact of the intervention was greater in Latinx persons and participants without primary care physicians.“Results of this cluster randomized clinical trial showed that with low NNT (number needed to treat), implementation of COVID-19 vaccine messaging platforms in EDs leads to greater vaccine acceptance and uptake in unvaccinated ED patients,” the researchers concluded. They added that broad implementation (of messaging) in EDs “could lead to greater COVID-19 vaccine delivery to underserved populations whose primary health care access occurs in EDs.”
Maybe they were looking for PACEMD's science?Yep, definitely good to keep those bowels clear. Nothing like a brisk flushing to keep the temperature down. Do a colonoscopy while you’re at it, 2 for 1.
Only very slight mortality in the dying group! Excellent result.
DanCar
Active Member
Are they calling to stop the shots are because most people now have natural immunity due to prior infection?You're confusing education with propaganda. If education had the effect you're claiming then more and more doctors would not be coming out calling to stop the shots.
Lets ask Dr Fukushima:Are they calling to stop the shots are because most people now have natural immunity due to prior infection?
Dr. Fukushima declared that “the harm caused by vaccines is now a worldwide problem” and that “given the wide range of adverse events, billions of lives could ultimately be in danger.”
Doesn't appear so. Also he appears to be quite upset.
PACEMD
Active Member
I think you meant you are confused by both education and propaganda. But that's ad hominem carelessness. You still haven't bothered to say one single thing verified as true. By omission verifying falseness. Crank up the chainsaw and ignore all reality..........the emperor has a new suit...........carry on...........You're confusing education with propaganda. If education had the effect you're claiming then more and more doctors would not be coming out calling to stop the shots.
Last edited:
Mask work?I think you meant you are confused by both education and propaganda. But that's ad hominem carelessness. You still haven't bothered to say one single thing verified as true. By omission verifying falseness. Crank up the chainsaw and ignore all reality..........the emperor has a new suit...........carry on...........
"If it disagrees with experiment, it’s WRONG. In that simple statement is the key to science. It doesn’t make any difference how beautiful your guess is, it doesn’t matter how smart you are, who made the guess, or what his name is… If it disagrees with experiment, it’s wrong. That’s all there is to it.”
Richard Feynman.
So I guess we can agree masks don't work now.
PACEMD
Active Member
Similar threads
- Replies
- 81
- Views
- 5K
- Replies
- 2
- Views
- 930
- Replies
- 165
- Views
- 25K
- Replies
- 85
- Views
- 9K
- Replies
- 23
- Views
- 5K
B