Thanks, I've been so confined to the house for the past year that I quickly turned a lobster-color even with copious SPF 45.

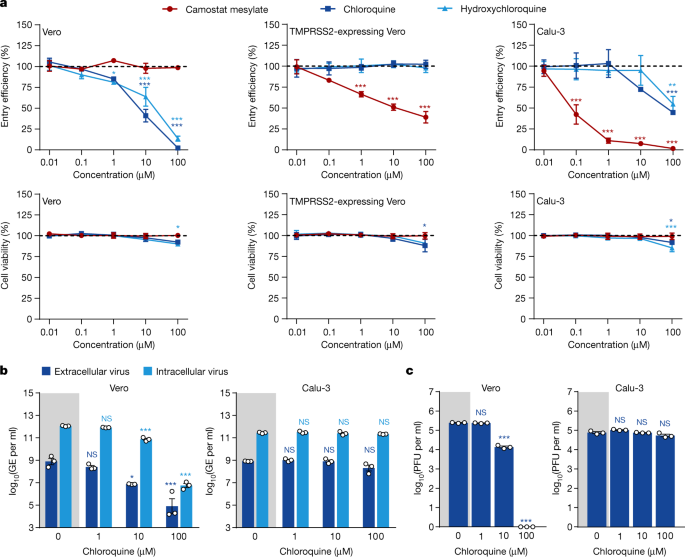
HEK cells are an "immortalized cell line" and have had so many genetic modifications to them that they do not represent much of anything SPECIFIC in the body anymore. They have been made into a "generic human cell" and I used them for years in the lab. They are GREAT for first pass experiments, but the problem with them is results in them do not always translate to other, more specific cell lines, or more importantly into organisms. HEK cells were appropriate for a "first pass" test to see if HCQ has any effectiveness in a test tube, but the lay public and politicians latched onto this like rabid animals and drew VERY inaccurate conclusions from the results, conclusions which no scientist would ever make. In fact that Nature article specifically points out that those results ONLY were valid in vitro (i.e. test tube - cell lines, etc.), and NOT in organisms, as the researchers should have.
Since that paper, there have been dozens of high-quality, randomized controlled trials in humans with HCQ . . . and low and behold it has panned out EXACTLY how it did when we tested HCQ against the influenza virus and other viruses decades again . . . like *sugar*. It doesn't do anything beneficial against ANY virus.
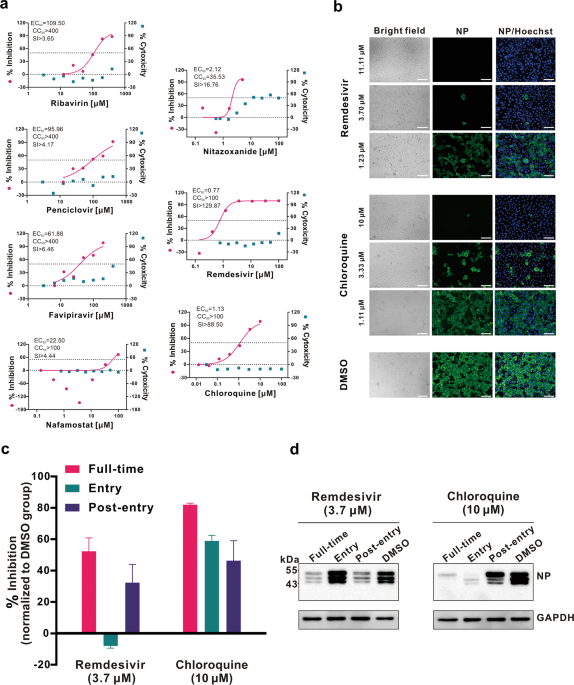
Remdesivir showed more promise early on, but long-term testing is showing that it is only really mildly effective, and probably best taken early in the course of mild disease if there is going to be any benefit.
There is another drug in testing showing promise (don't remember the name), but it still should be viewed as far inferior to getting vaccinated. The vaccines are in about 100 million people now, and have shown incredibility safe side effect profiles. Honestly, modern miracles in the time-frame they were built, tested, and distributed.



 apnews.com
apnews.com