bkp_duke
Well-Known Member
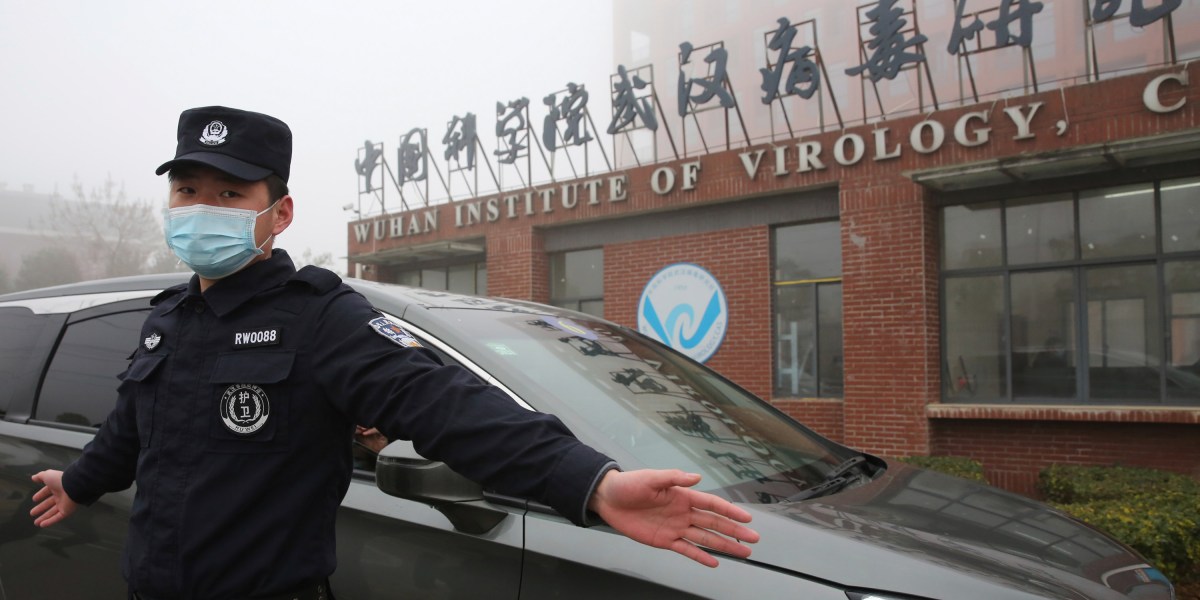
This annoys me tremendously because I'm having to enter medical facilities these days to get some treatment for my shoulder. It should be a nearly perfectly safe environment at this point (patients are kept well isolated from one another), but it sounds like it's not.
Seems like the third/fourth surge is just beginning. It seems to be coming perhaps a week later than predicted by models (though that could be due to the models providing day of symptoms and the surge being the day of report).
We'll see how bad it is (I expect we'll remain below 100k for the 7-day average, which is quite high but depends on the age distribution). I'm still optimistic that in many states it's going to end up being very mild due to immunity from infection and vaccination. Just have to keep a close eye on those hospitalizations as the cases spike. I expect the surge will be largely cut off and brought to a halt by late April, regardless. At that point there should be just too much immunity to support a massive outbreak.
It's bad news for school reopening, of course. We really want minimal community spread and very low baseline levels for that to avoid having children killing their parents with the virus. The resumption of spread is not going to make successful reopening easier. Still no talk of rapid tests.
It's actually the opposite. Since the beginning of the pandemic, 1 in 6 infections have been healthcare workers or their families. Assuming they know how to use PPE (most do), this really speaks volumes of just how infectious this virus is.