


Norbert
TSLA will win
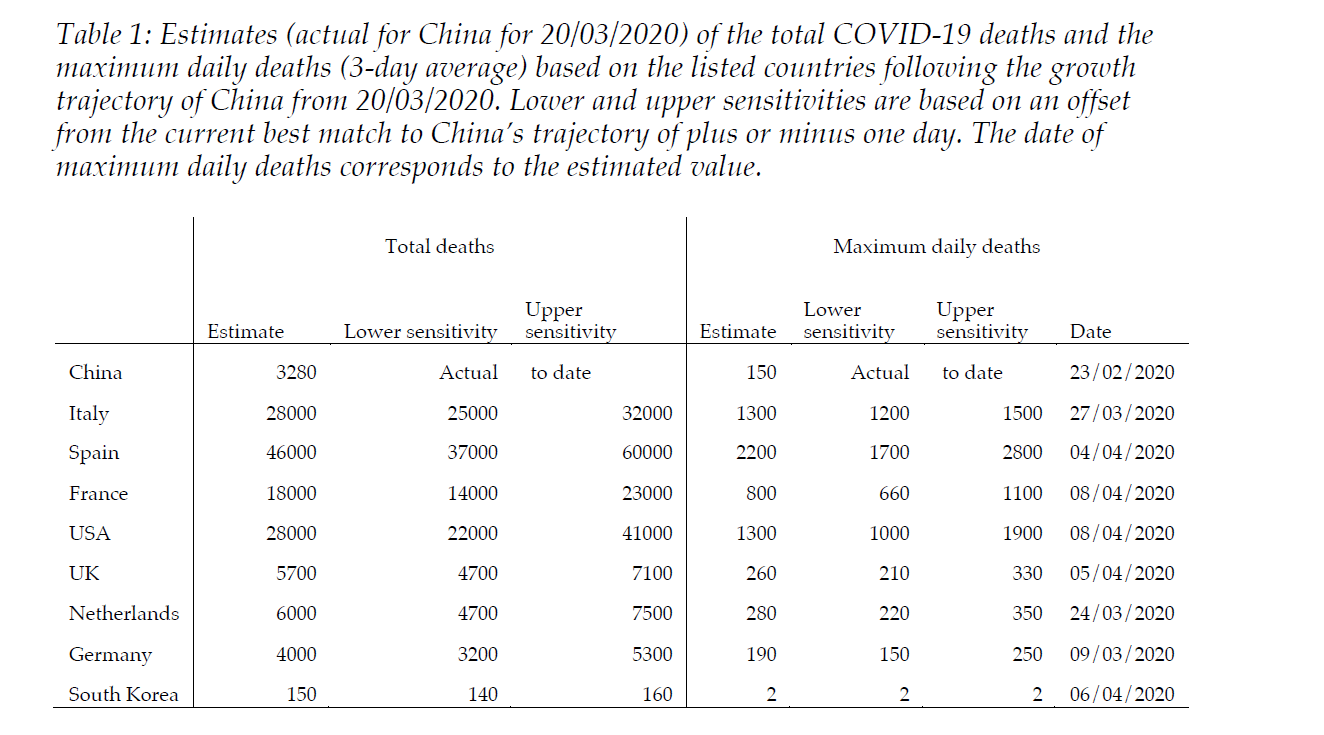
I hate to say it but as far as I can tell with the current death rate and trajectory in Italy a fatality rate in the range of 200-500 DPM in the relatively short term is a near certainty. It could even be higher with the hospitals completely overwhelmed in some areas. The only thing I can see that will stop that is some miraculous treatment breakthrough in the very short term, which seems highly unlikely. One crude model I posted recently estimated that deaths in Italy would be in the range of 25000-32000, which would put the DPM at the high end of your range, and it is not clear this model adequately factors in the added fatalities from an overwhelmed medical system. https://www.medrxiv.org/content/10.1101/2020.03.25.20041475v1.full.pdf
I would appreciate your thoughts about this as I have great respect for your modeling, and I'm basically spitballing here.
The reason I am interested in IFR and/or serological testing is to have some sense of where we will be in different parts of the world after social distancing and other policies have taken effect and the virus is under control at least temporarily. Will 50% of the population already be exposed and herd immunity in effect, or will we barely be scratching the surface with only 1-5% exposed? That's a critical question and we don't seem to have a clue.
One of the problems with deciding how to tackle this virus or plan for it is that almost all of the attention is focused on the short term (understandable in a crisis but still a problem). We lack the most basic information necessary to predict how things will play out in the medium to long term. If we tamp it down in the next couple months in the Northern hemisphere, is it going to come roaring back with equal or greater force after we lift restrictions, or next winter (assuming it is temperature sensitive -- IMO probably yes but another issue where the jury still seems to be out).
A problem with drawing conclusions from the US trajectory of tested cases, is that it is too much determined by testing capacity.
