


EVNow
Well-Known Member
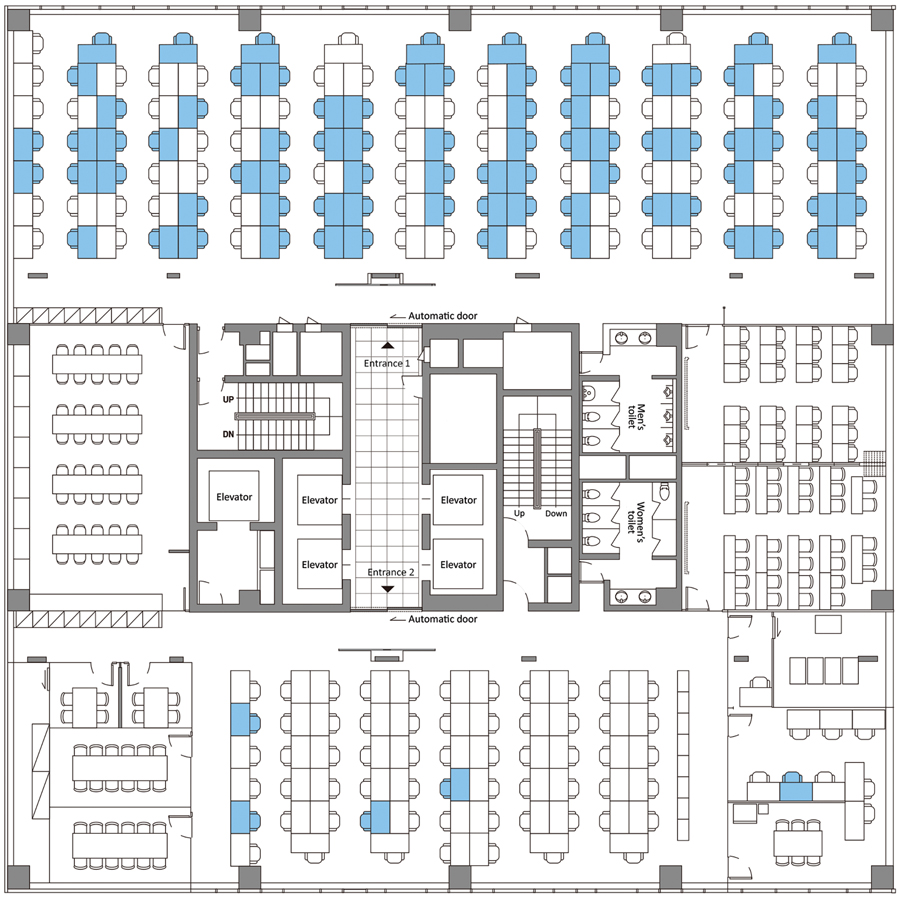
Open seating office is the worst for Covid containment.
Early Release - Coronavirus Disease Outbreak in Call Center, South Korea : COVID19
Early Release - Coronavirus Disease Outbreak in Call Center, South Korea : COVID19
