That’s great, you can make that choice and I’m glad it worked out. Many countries do not recommend it. The WHO says there is no evidence healthy children or teens need a booster. CNBC link So it is not at all fringe or misinformation for parents to question it (especially second doses of mRNnA...

teslamotorsclub.com
Just before Omicron took off, vaccines available for some children.
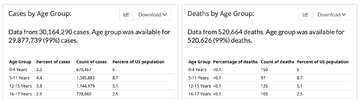
Cases: 8.67million
Deaths: 1133
CFR: 1 in 7653
Total Now:
Cases: 16.644million
Deaths: 2145
Incremental (Entire Omicron era with vaccines available ):
Cases: 7.97 million
Deaths: 1012
CFR: 1 in 7875
Caveats:
1) deaths are removed from counts sometimes by CDC so initial numbers and current numbers are slightly higher than actual. Minimal impact on results.
2) Cases only. Ascertainment rates have of course changed a significant amount (but note ascertainment has always been a problem, so likely overall decrease in ascertainment is probably down by factor of 3 at most, identifying maybe 1 in 5 cases - note that there are 16 million cases on a pop of 70mil so that is 1 in 5 so clearly ascertainment can’t be worse than that!).
3) All the other caveats discussed here which we all know now.
I think it is a pretty fantastically poor performance to see no change in CFR with a “more mild” Omicron and with vaccines available. Likely IFR is down by a factor of 2 or 3 or so. Pretty bad. Still 1 in 10k kids identified with COVID dies (hard to know exact current incremental rate; would have to look at a more recent post of mine with the datapoint to calculate the slope).
Note that about the same number of children have died from Omicron as died from Delta and the OG virus.
Worth nothing that 0-4,
the age group affected by the booster dose post that started this discussion, is
by far the most vulnerable to COVID in age groups under 18. I think these data would suggest it is extremely advisable for parents to get their tots vaccinated, whatever about older children.